
Supracondylar fractures of the humerus are the most common type of elbow fractures in children and adolescents. This is because the end of the humerus bone, just above the joint and the growth plates, is wafer-thin. Though fractures of this “supracondylar” region heal quickly, they are relatively unstable (i.e. they tend to displace under the pull of muscles, primarily the Triceps) and frequently require operative stabilization.
Treatment of pediatric supracondylar humerus fractures depends on the amount of initial or subsequent angulation and/or displacement. Type I is a non-displaced fracture that does well in a long arm cast for 3-4 weeks. Type II are angulated fractures that can sometimes be managed in a cast, but frequently require surgery. Type III fractures universally require operative intervention because of their displaced nature.
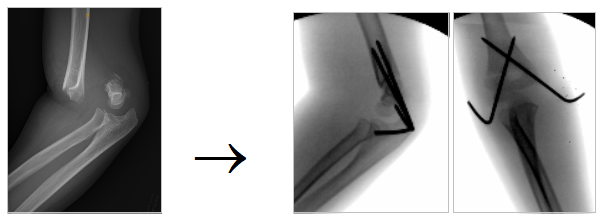
Surgical intervention for these elbow fractures consists of “Closed Reduction and Percutaneous Pinning”. With the child asleep under general anesthesia (and please note that safe induction of anesthesia requires an empty stomach), the fracture can usually be “set” into place. However, because of the tendency for the bones to shift if only put into a cast, they are stabilized by “pins”. Two to three small diameter, smooth stainless steel wires are poked through the skin to stabilize the bones. A cast is then put on while the child is still under anesthesia. The procedure generally takes less than an hour. Pin-related infections are uncommon (<1%) as the procedure is done in the clean environment of the operating room and one dose of antibiotics is given in the operating room (none are required after). The first time you will see the pins will be when they are painlessly removed in the office after the fracture has healed (generally 4 weeks after surgery).